
Diabetes Mellitus (DM) is a worldwide menace which has no boundaries. Its prevalence is increasing at epidemic proportions. There are over 150 million people affected by DM worldwide and this number is expected to be doubled by 2025. The number of Americans effected has grown to 24 million (approximately 8% of the population), according to the Centre for Disease Control (CDC) and Prevention’s 2007 Diabetes Fact Sheet. It also is estimated that another 57 million people have pre-diabetes which puts them at increased risk for the disease.
DM can affect almost every organ in the body. If not controlled well it may eventually lead to heart attack, stroke, kidney failure and blindness. It is the 7th leading cause of the death in the USA.
DM type 1 is more prevalent in people who are younger than 30 years old, lean and have absolute insulin deficiency. They require insulin for therapy. DM type 2 is usually found in adults more than 30 years of age. They are generally obese individuals who have insulin resistant and partial insulin deficiency. DM type 2 accounts for 90 percent of all diabetics. Prevalence of obesity is one of the main reasons for DM aside from poor diet control and family history of DM. The ethnic groups that are hardest hit by diabetes: African-Americans, Hispanics, American Indians, and Asian/Pacific Islander – have been growing.
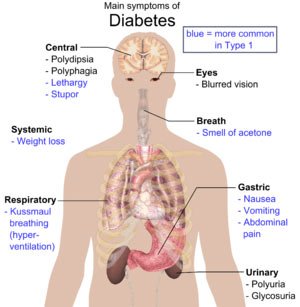
DM is defined as fasting blood sugar (BS) of more than 126 on two occasions. It can be confirmed if BS is more than 200mg/dl two hours after ingestion of 75 gm of carbohydrate. Symptoms of diabetes are excessive thirst, urination, hunger and unexplained weight loss.
The care of these patients require close coordination between the physician, nurse, dietician and diabetic educator. Patient must be given comprehensive education about their disease, monitoring of BS, and complications. Maintaining good control of blood sugar is paramount in avoiding the long term future complications.
Beside regular BS check, patients should be monitored for hemoglobin A1C every 3-6 months, urine albumin level, fasting lipid profile, close foot exams and yearly ophthalmology follow-up.
Currently only one-half of the people with diabetes have been diagnosed. The screening for DM should begin at 45 years of age and should be repeated every three years in persons without risk factors. Those patients with risk factor should be tested more often. Risk factors include obesity, first degree relatives with diabetes mellitus, hypertension, hyperlipidemia or previous evidence of impaired glucose homeostasis. Earlier detection may lead to tighter control of blood glucose levels and a reduction in the severity of complications associated with this disease.
A 2006 report by Harvard Medical School noted that 90% of cases of diabetes could be prevented with healthy diet and lifestyle changes including exercise such as walking 30 minutes per day. Healthy diet should include high fiber, fruits, vegetables, lean meat , poultry and fish.
Use of Aspirin and a low protein diet are important. Use of angiotensin converting enzyme inhibitor and angiotensin receptor blocker and direct renin inhibitor reduces the development and progression of kidney disease.
Therapy protocol for Type II includes use of either Metformin or TZD (thiazolidinediones) in combination with another oral hypoglycemic agent is the initial therapy. Use of long active insulin such as insulin detmir or insulin glargine, are being considered much earlier than in the past. Use of these insulin’s serve to control BS sooner and have less hypoglycemic episodes than other agents. According to the May 24, 2008 issue of Lancet, patients with diabetes who took long acting insulin soon after diagnoses had better control of their blood sugar level. According to this study, researcher’s in China found that blood sugar levels in at least 95% of insulin users dropped to normal in fewer than six days.
Treatment for Type 1 is mainly lnsulin therapy. Pancreatic transplant is recommended for DM type I patients with poor kidney function. Usually the best option happens to be Simultaneous Pancreas Kidney transplant rather than Pancreas Transplant alone. This procedure involve transplanting of Islet cell ,but not entire organ in donor’s body. Although organs from about 7000 deceased donors become available each year in the US, fewer than half of the donated pancreas is suitable for whole organ transplantation or harvesting of the islets cell ,enough for only a small percentage of those with Type I DM.
DM is a grave disease which should be taken very seriously. Even a little effort on patient’s part such as regular exercise, healthy diet and control of obesity can go a long way in postponing the onset of disease for many years. Continued vigilance and combined research efforts are required to combat this worldwide menace.
[Dr. Anis Ansari is a board certified nephrologist, practising at Medical Associate in Clinton, IA, USA]